The Problem with the Food Frequency Questionnaire
I’ve made no secret that I don’t like Food Frequency Questionnaires. (FFQ). I understand why they are used; when a study may contain 500, 5,000, or 500,000 subjects, to do a dietary recall of the prior 24 hours, using a dietician to help determine portion sizes, would be close to impossible or very difficult at best. When nutritional research became the focus of examining dietary intake in populations across all ages, genders, and ethnic groups, the FFQ was developed. It was developed for the myriad studies of healthcare professionals; the first time I recall its use was the Women’s Health Initiative. Those studies have been going on for close to 50 years or more with repeated measures every few years.
Until very recently, they’ve used the exact same form of the FFQ that was developed 50 years ago. Because we covered studies on meat intake, let’s look at how the FFQ assesses intake of unprocessed meat. I’ll use only one item as an example: Hamburger (1 patty)
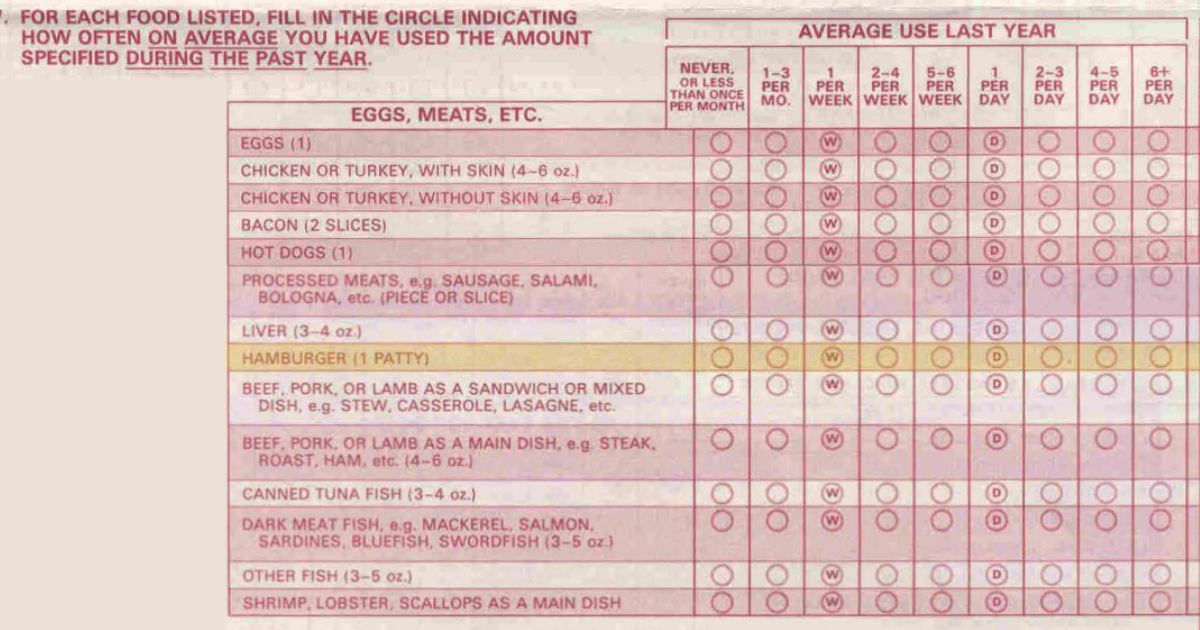
The problem with this particular choice is that it doesn’t define what makes a patty either by grams or ounces. While I know that things have changed as it relates to our red meat intake, very few of us ever ate more than six hamburgers per day.
Those intake categories across the top apply to every food on the questionnaire. So tell me: how many fresh pears did you eat in 2023? How many tablespoons of jam or jelly? How can anyone answer these questions accurately?
It seems that this questionnaire was made in an era where people had more standardized food intake than they do today, although even back in the 1980s, the concept of family breakfast, lunch, and dinners seemed on its way out. These days we snack and graze, which makes it even harder to remember what we ate.
On Saturday, I’ll wrap this up on why the FFQ may provide a direction but isn’t precise enough to associate diet with disease in my opinion.
What are you prepared to do today?
Dr. Chet
Reference: https://nurseshealthstudy.org/participants/questionnaires